A washout period in clinical trials may sound technical and even intimidating at first.
You finally find a clinical trial that feels like a potential option. It may offer access to a new investigational treatment, closer monitoring, or another path to explore. You scroll through the eligibility details and then you see a line that makes you pause.
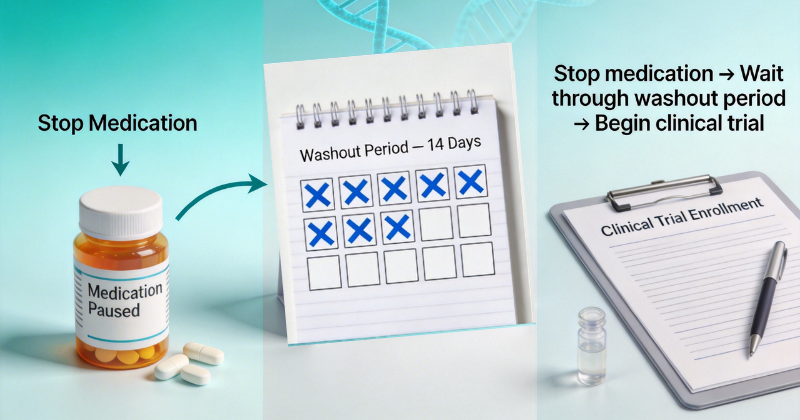
“Participants must complete a 14-day washout period before enrollment.”
Suddenly, questions start racing.
Do I need to stop my current medication?
Is that safe?
Will I still qualify?
If you are considering trial participation, understanding the washout period can help you make informed and confident decisions. This guide explains what is a washout period in clear, simple language without overwhelming medical jargon.
What is a Washout Period?
A washout period is a planned amount of time during which a participant stops taking certain medications before starting a clinical trial.
In simple terms, it is a clearing period that allows previous drugs to leave your body before a new study treatment begins.
Educational resources explain that a medication washout helps ensure earlier treatments do not interfere with study results. Major clinical research registries include washout periods as part of official trial protocol terminology, highlighting how standardized this process is in research.
The washout period is not random. It is carefully calculated and built into trial participation requirements to support both safety and accurate study results.
Why a Washout Period Matters in Clinical Trials
Clinical trials must produce reliable data. If someone begins a study while another medication is still active in their system, researchers may not know which drug is responsible for:
- Improvements
- Side effects
- Lab changes
- Symptom differences
Federal clinical trial design guidance emphasizes controlling variables in research studies to ensure reliable results. A washout period helps reduce overlapping drug effects and improves clarity in study outcomes.
Washout periods are particularly important in:
- Early clinical trial phases such as Phase 1 and Phase 2
- Trials testing new drug classes
- Studies measuring specific symptom or laboratory changes
Without a proper washout period, results may become difficult to interpret.
How Drug Clearance Time Works
To understand the washout period, it helps to understand drug clearance time.
Every medication has something called a half-life. A half-life is the time it takes for half of a drug to leave your bloodstream.
For example:
- If a drug has a 24-hour half-life, after 24 hours only 50 percent remains.
- After another 24 hours, 25 percent remains.
Most medications require about 4 to 5 half-lives to be mostly cleared from the body. This is why washout period timelines differ from one medication to another.
A medication washout may last:
- 48 hours
- 1 to 4 weeks
- Longer for long-acting medications
Drug clearance time depends on:
- Liver and kidney function
- Dosage
- Duration of use
- Individual metabolism
The washout period is based on pharmacology and safety science and not guesswork.
5 Essential Facts About a Medication Washout
1. A Washout Period Protects Your Safety
The primary purpose of a washout period is safety.
Stopping one medication and immediately starting another could increase the risk of:
- Drug interactions
- Unexpected side effects
- Altered treatment response
The washout period gives your body time to stabilize before introducing the investigational treatment.
2. Not Every Trial Requires a Washout Period
Some studies allow stable background medications.
Others require a medication washout only for specific drug categories.
Washout requirements depend on:
- The condition being studied
- The investigational therapy
- Clinical trial phases
- Trial participation requirements
Reviewing eligibility criteria carefully is important before expressing interest.
3. You Will Not Be Asked to Stop Medication Without Medical Supervision
A washout period does not mean stopping medication on your own.
If a medication washout is required:
- The research team evaluates your safety
- Your treating physician may be consulted
- A tapering plan may be created if needed
- Monitoring is provided
Participant safety is always the top priority in ethical clinical research.
4. Washout Periods Can Affect Scheduling
A washout period may impact when you can officially enroll.
It might:
- Delay study start by 1 to 4 weeks
- Require additional screening visits
- Include lab testing before and after drug clearance time
If you are balancing work, family responsibilities, or caregiving, knowing this timeline early helps you plan realistically.
5. Washout Requirements May Affect Clinical Trial Eligibility
In some cases, washout timing determines whether you qualify.
For example:
- If your medication cannot be safely stopped
- If symptoms worsen during the washout period
- If enrollment closes before your medication washout ends
These factors can influence clinical trial eligibility.
Clear eligibility disclosure helps you avoid surprises.
Washout Periods and Clinical Trial Phases
Washout periods are more common in early clinical trial phases, especially Phase 1 and Phase 2.
In Phase 1 studies, researchers are often studying a drug in humans for the first time. Because of this, investigators want to make sure that no other medications are influencing the results. A washout period helps create a clean starting point so researchers can understand how the investigational drug behaves in the body.
Phase 2 trials also frequently use washout periods. These studies focus on how well a treatment works for a specific condition and what side effects might occur. If previous medications remain active in the body, it becomes difficult to determine whether improvements or side effects are related to the study treatment.
In later Phase 3 trials, researchers may sometimes allow background medications depending on the study design and the condition being studied. By this stage, the treatment has already been studied for safety and dosing. Researchers may focus more on comparing the treatment with existing therapies or evaluating how it performs in larger groups of patients.
Even in Phase 3 trials, however, washout periods may still be required for certain medications that could interfere with the study results. Each trial defines its own washout requirements based on the treatment being studied, the condition involved, and participant safety considerations.
Final Thoughts: Making Confident Decisions About a Washout Period
A washout period is not meant to create barriers. It exists to protect your safety and ensure accurate scientific results.
Understanding what is a washout period, how drug clearance time works, and how medication washout affects clinical trial eligibility empowers you to ask informed questions:
- Is it safe for me to pause my medication?
- How long will the washout period last?
- How does it affect my schedule?
- What are the full trial participation requirements?
After checking eligibility details, always discuss any potential trial and its washout requirements with your treating doctor before making changes to your medication.Clinical research depends on informed volunteers. When the washout period and eligibility criteria are clearly explained, participation becomes a thoughtful decision and not a confusing one.
Wondering what a washout period means for your schedule? Find transparent, clearly explained trials on DecenTrialz.